Statin Therapy and Risk of Acute Exacerbations in Adults With Mild Asthma
Background
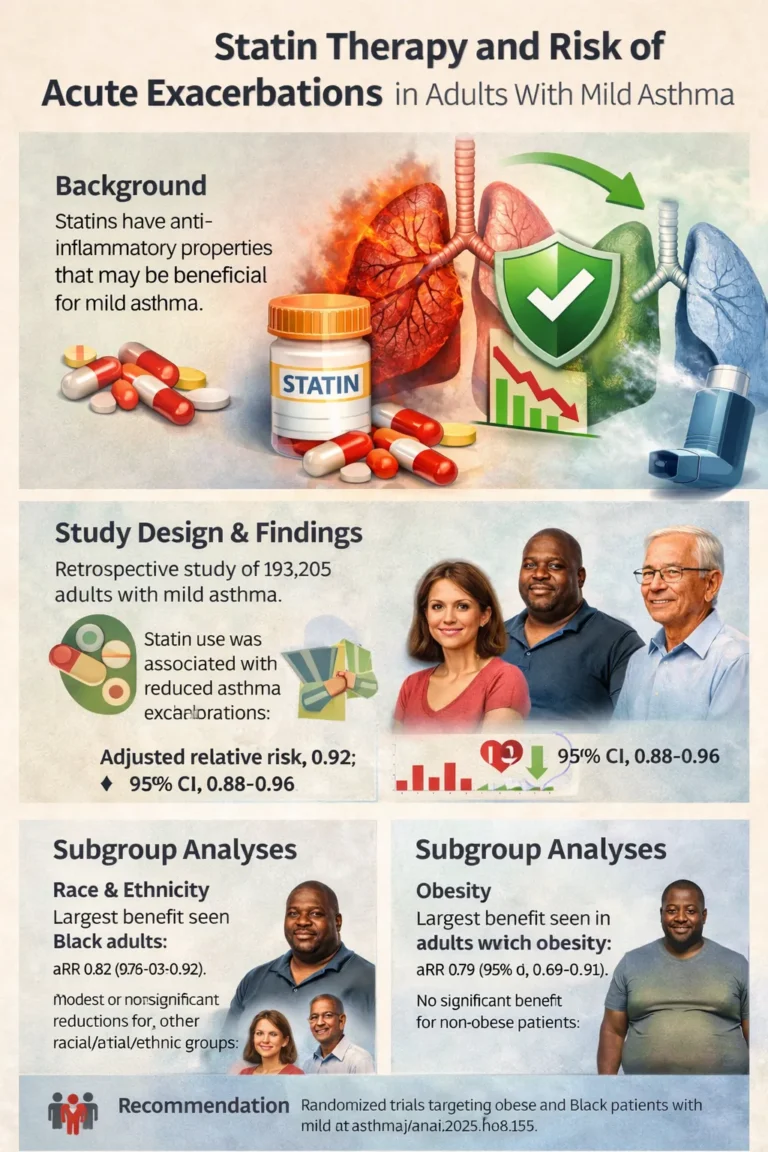
Statins, widely prescribed for cardiovascular disease prevention, exhibit pleiotropic effects that extend beyond lipid lowering. Their anti-inflammatory and immunomodulatory properties have generated interest in their potential therapeutic role in chronic inflammatory airway diseases, including asthma.
Prior investigations examining statins in asthma have produced heterogeneous findings, with some studies demonstrating benefit and others reporting null effects. Clarifying which patient subgroups may derive clinical benefit is therefore essential in determining the potential role of statins in asthma management.
–
Study Design and Population
In this retrospective cohort study, investigators evaluated 193,205 adults with mild asthma receiving care within Kaiser Permanente Southern California.
The cohort had a mean age of 43.8 years; 64.2% were women. The racial and ethnic distribution included:
* 39.4% Hispanic
* 37.6% White
* 12.8% Black
* 10.3% Asian/Pacific Islander
The primary outcome was risk of acute asthma exacerbation during the year following statin dispensation.
Overall Findings
After adjustment for relevant covariates, statin use was associated with a statistically significant reduction in the risk of acute asthma exacerbations:
* **Adjusted relative risk (aRR): 0.92**
* **95% CI: 0.88–0.96**
According to Crawford,
> “Patients with mild asthma are indeed less likely to suffer an asthma attack if they have been dispensed a statin medication in the prior year compared to patients with mild asthma who have not received a statin medication.”
Subgroup Analyses
Race and Ethnicity
When stratified by race and ethnicity, the protective association was significant only among Black patients
* **Black patients:** aRR 0.82 (95% CI, 0.73–0.92)
* Hispanic, White, Asian/Pacific Islander patients: modest but nonsignificant reductions no
Crawford noted:
> “Interestingly, this finding was most apparent among obese patients and among Black patients.”
However, investigators advised caution in interpreting these subgroup findings, acknowledging potential differences in asthma phenotypes, access to care, and medication adherence patterns across demographic groups.
—
Body Mass Index
When analyzed according to BMI:
* **Patients with obesity:** aRR 0.89 (95% CI, 0.84–0.94)
* Normal weight, underweight, overweight: nonsignificant associations
The greatest risk reduction was observed among Black patients with obesity:
* **Black patients with obesity:** aRR 0.79 (95% CI, 0.69–0.91)
* Non-Black patients with obesity: aRR 0.90 (95% CI, 0.85–0.96)
* Patients without obesity (Black and non-Black): no significant benefit
Crawford stated:
> “This finding is significant because it suggests that future randomized controlled trials of statin use in asthma may be most effectively targeted towards cohorts of obese and/or Black patients.”
Mechanistic Considerations
Statins have demonstrated anti-inflammatory properties that may influence airway inflammation, a shared pathogenic pathway between asthma and cardiovascular disease. Crawford emphasized:
> “Multiple reports in the literature suggest that statins possess anti-inflammatory properties that may make them beneficial for conditions other than the cardiovascular diseases for which they are traditionally used.”
The investigators were particularly interested in determining whether statin use correlated with fewer asthma exacerbations in their large and diverse population:
> “We also wondered whether certain sub-populations of patients with mild asthma would be more likely than others to have improved asthma outcomes associated with statin use.”
—
## Clinical Implications
The findings suggest a potential adjunctive pharmacotherapeutic role for statins in select populations with mild asthma, particularly among patients with obesity and Black patients.
Crawford observed:
> “Doctors may consider prescribing statins to patients with both cardiovascular disease and asthma.”
He further noted that informing patients of possible respiratory benefits could improve adherence:
> “Such patients should be advised that further research needs to be done to verify that statin use is indeed beneficial for asthma.”
Importantly, statins should not currently be prescribed solely for asthma management.
—
Perspective
Blen Tesfu, MD, General Practitioner (Welzo, London), commented that the findings are biologically plausible given the inflammatory overlap between cardiovascular disease and asthma. He suggested that statins may provide secondary benefits beyond their intended use.
Clinical observations have noted stabilized asthma symptoms in some patients receiving statins for cardiovascular indications, although these reports remain anecdotal.
Tesfu emphasized that:
* Statins remain primarily indicated for cardiovascular prevention.
* There is no current justification for prescribing statins specifically for asthma.
* The findings provide reassurance when statins are indicated for cardiovascular disease in patients who also have asthma.
—
Future Directions
Crawford recommended large, adequately powered randomized controlled trials comparing statins with placebo in patients with asthma and cardiovascular disease. These trials should:
* Stratify participants by obesity and race
* Follow subjects for at least 1 year
* Assess exacerbation frequency and adverse events
* Include sufficient sample size to detect differences in relatively infrequent outcomes
He stated:
> “Subjects should be followed for at least 1 year to determine the frequency of asthma exacerbation in both the treatment and placebo groups as well as to detect any potential adverse effects of statins vs. placebo when used for the treatment of asthma.”
Further research should also clarify whether observed associations are causal and identify specific asthma phenotypes most likely to benefit.
—
Conclusion
In a large retrospective cohort of adults with mild asthma, statin use was associated with a modest but statistically significant reduction in acute exacerbations, particularly among Black patients and patients with obesity. While these findings suggest a potential adjunctive role for statins in selected populations, randomized clinical trials are required before changes to asthma management guidelines can be recommended.
Source Information Crawford W, et al. Ann Allergy Asthma Immunol. 2025; doi:10.1016/j.anai.2025.08.159


{kind=link}