High Prevalence of Hypercortisolism in Patients With Resistant Hypertension: Findings From the MOMENTUM Study
Importance Resistant hypertension affects a substantial proportion of patients with elevated blood pressure, yet the underlying secondary endocrine causes—such as hypercortisolism—often remain underdiagnosed. Identifying these hidden etiologies is critical for appropriate referral and targeted management.
Objective To determine the true prevalence of endogenous hypercortisolism among a large cohort of patients diagnosed with resistant hypertension.
Design, Setting, and Participants The MOMENTUM study, presented at the American College of Cardiology (ACC) Scientific Session in New Orleans, evaluated 1,086 patients with resistant hypertension. Resistant hypertension was strictly defined as either maintaining a systolic blood pressure of 130 mm Hg or higher despite adherence to at least three classes of antihypertensive medications (including a diuretic), or requiring at least four classes of antihypertensive medications (including a diuretic) regardless of current blood pressure control.
Patients were screened for endogenous hypercortisolism utilizing a standard dexamethasone suppression test. A positive diagnosis was established if cortisol levels remained greater than 1.8 µg/dL in the presence of dexamethasone levels of at least 140 ng/dL.
Table 1. Diagnostic Criteria in the MOMENTUM Study
| Diagnostic Category | Clinical Criteria |
| Resistant Hypertension | Systolic BP $\ge$ 130 mm Hg on $\ge$ 3 antihypertensive classes (including a diuretic)
OR
Use of $\ge$ 4 antihypertensive classes (including a diuretic) regardless of BP. |
| Endogenous Hypercortisolism | Positive dexamethasone suppression test: Cortisol > 1.8 µg/dL with dexamethasone $\ge$ 140 ng/dL. |
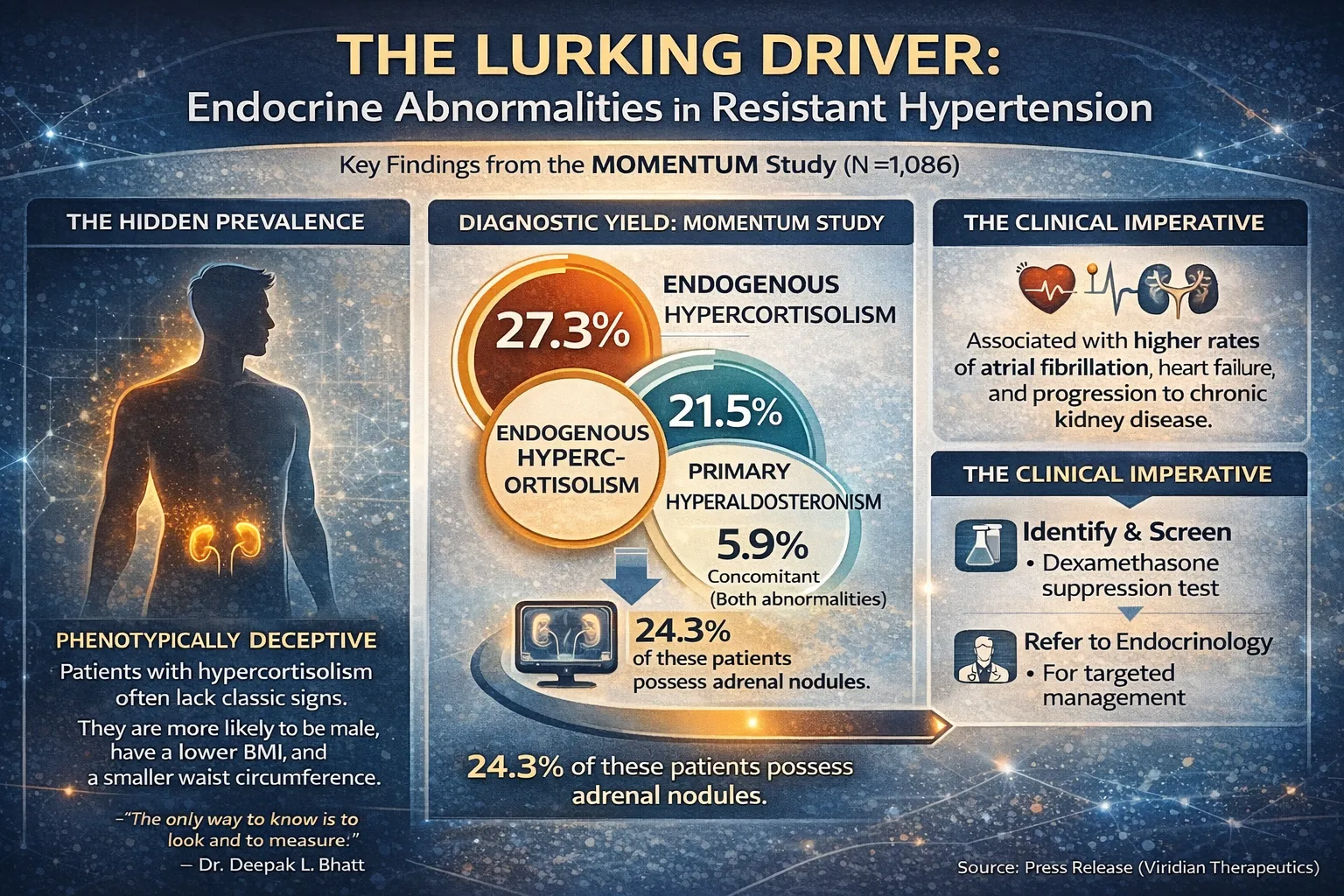
Main Outcomes and Results The study revealed that endogenous hypercortisolism is highly prevalent in this population, affecting more than one in four patients. Specifically, 27.3% (95% CI, 24.7%-31.1%) of the resistant hypertension cohort tested positive for hypercortisolism. Furthermore, primary hyperaldosteronism was identified in 21.5% of the cohort, with an overlapping 5.9% of patients testing positive for both endocrine abnormalities. Among the subset of patients with confirmed hypercortisolism, 24.3% were found to have adrenal nodules upon subsequent CT imaging.
Deepak L. Bhatt, MD, MPH, MBA, director of the Mount Sinai Fuster Heart Hospital, contextualized the magnitude of these findings: “The purpose of the study [was] to see what the prevalence is of real hypercortisolism in this patient population of folks with resistant hypertension, which is a pretty common population; somewhere between 10% and 15% of patients in that large universe of hypertension have resistant hypertension.” He added, “Unlike what I think lots of doctors believe, it was extremely common.”
Table 2. Prevalence of Endocrine Abnormalities in the Resistant Hypertension Cohort (N = 1,086)
| Endocrine Abnormality | Prevalence (%) | 95% Confidence Interval |
| Hypercortisolism | 27.3% | 24.7% – 31.1% |
| Primary Hyperaldosteronism | 21.5% | — |
| Concomitant Hypercortisolism & Hyperaldosteronism | 5.9% | — |
| Adrenal Nodules(among hypercortisolism-positive patients) | 24.3% | — |
Phenotypically, patients with hypercortisolism deviated from classic expectations. When compared to those without the condition, hypercortisolism-positive patients were more likely to be male and notably possessed lower body mass indices (BMI) and waist circumferences. However, this subgroup exhibited numerically higher rates of significant cardiovascular and metabolic comorbidities, including atrial fibrillation, coronary artery disease, heart failure, and suboptimal glycemic control. Furthermore, hypercortisolism was associated with poorer baseline kidney function and an elevated risk for progression to chronic kidney disease.
Conclusions and Relevance The MOMENTUM study demonstrates that endogenous hypercortisolism is a common, “lurking” driver of resistant hypertension that frequently presents without the classic, observable stigmata of Cushing’s syndrome.
Dr. Bhatt emphasized the limitations of relying on visual assessment alone: “Another message here is that hypercortisolism within the population of resistant hypertension is quite prevalent. It’s lurking, and it’s not so obvious that you just look at the patient and say, ‘Oh, that one has hypercortisolism.’ So yes, one should be vigilant for things like signs of Cushing’s syndrome, but that’s not really at all what we’re talking about here. We’re talking about endogenous hypercortisolism, but without necessarily having those obvious features that any medical student would be trained to detect. What it means is that we can’t just rely on those classic physical exam findings that we memorized in medical school to identify cortisol excess. Within a resistant hypertension population, at least, the only way to know is to look and to measure.”
The clinical imperative is systematic screening and subsequent multidisciplinary referral.
“The message from MOMENTUM is to screen patients with resistant hypertension for hypercortisolism [and] also for hyperaldosteronism,”
stated Dr. Bhatt. He advised that upon identifying endogenous hypercortisolism, “the next best step is probably to refer to an endocrinologist for further management of that… The key is for those types of physicians [primary care and cardiologists] to identify and then refer, most likely to an endocrinologist.”
Endocrine Drivers in Resistant Hypertension
Prevalence Data from the MOMENTUM Study Cohort (N = 1,086)

{kind=link}