Early Cardiovascular Risk in Lupus: Insights from the 2025 AWIR Conference**
Cardiovascular disease (CVD) is one of the most serious and prevalent causes of death among individuals with systemic lupus erythematosus (SLE). According to Dr. Maria Dall’Era—chief of rheumatology at the University of California, San Francisco and director of the UCSF Lupus Clinic—organ damage in lupus begins early and contributes significantly to both morbidity and mortality. She emphasized this point during her presentation at the 2025 Association of Women in Rheumatology (AWIR) annual conference.
> “Cardiovascular disease and damage is a leading cause of mortality in SLE,” Dall’Era stated.
### **A Long-Recognized Risk—Now Understood to Begin Early**
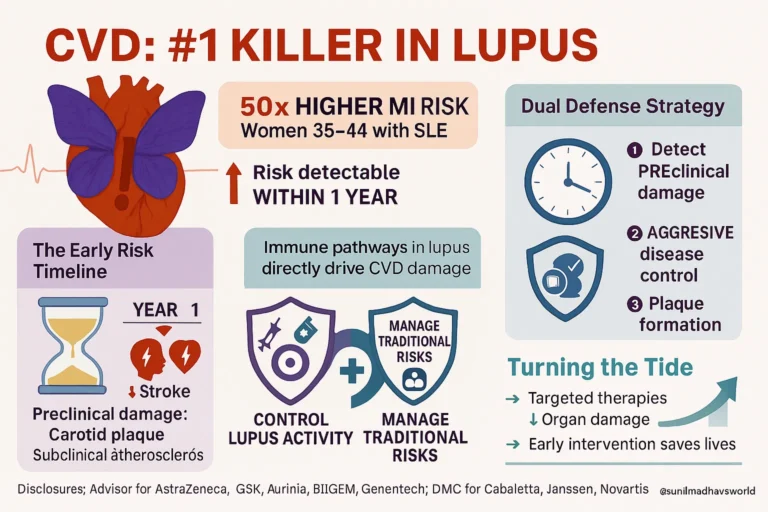
While it has long been known that lupus patients face elevated cardiovascular risk, recent research has shifted the timeline of concern. Historically, cardiovascular complications were considered late-stage manifestations of lupus. However, new data show that events such as myocardial infarction and stroke can occur much earlier—sometimes within the first year of diagnosis.
> “Even at 1 year we see an increase in cardiovascular risk in our lupus patients,” Dall’Era noted.
One particularly alarming statistic: women with lupus between the ages of 35 and 44 have a 50-fold increased risk of heart attack compared to their peers without lupus. Traditional cardiovascular risk factors—such as high blood pressure, cholesterol abnormalities, and obesity—do not fully explain this elevated risk. Instead, lupus-specific immune mechanisms appear to play a major role.
> “Many of the immune pathways that play a role in cardiovascular risk are also operative in lupus,” she explained.
### **The Challenge: Detecting and Preventing Early Damage**
Dall’Era stressed the importance of identifying the preclinical phase of cardiovascular damage in lupus—when patients may already be developing carotid plaque or subclinical atherosclerosis, even in the absence of symptoms. The challenge for rheumatologists is to intervene before this damage progresses.
> “How do we get on top of that and prevent worsening?” she asked.
### **Strategies for Reducing Cardiovascular Risk in Lupus**
To address this challenge, Dall’Era outlined a multifaceted approach:
– **Routine Cardiovascular Screening**: Regular monitoring for blood pressure, lipid abnormalities, and atherosclerotic plaque formation is essential.
– **Lifestyle Management**: Supporting patients in managing sleep quality, weight, and other modifiable lifestyle factors can help reduce cardiovascular risk.
– **Disease Activity Control**: Achieving remission or maintaining a low disease activity state—defined by frameworks such as DORIS (Definition of Remission in SLE) or LLDAS (Lupus Low Disease Activity State)—has been shown to reduce plaque formation and vascular damage.
> “You can bring down the risk,” Dall’Era emphasized.
She also highlighted the importance of a treat-to-target approach and disease modification as central goals in lupus management. Advances in understanding the molecular mechanisms of SLE and lupus nephritis are enabling clinicians to use targeted therapies more strategically to control disease activity and prevent organ damage.
> “There are things that we can do to begin to mitigate this progression of cardiovascular disease in our patients,” she said. “We still have a lot of work to do, but we are moving in the right direction.”
—
### **Source & Disclosures**
This presentation was part of the 2025 AWIR annual conference held July 24–26 in Orlando, Florida. Dr. Dall’Era disclosed advisory roles with AstraZeneca, GlaxoSmithKline, Aurinia, Biogen, Bristol Myers Squibb, and Genentech, and participation on data monitoring committees for Cabaletta, Janssen, and Novartis.

{kind=link}
No comments yet. Start the discussion!